
Партнерка на США и Канаду по недвижимости, выплаты в крипто
- 30% recurring commission
- Выплаты в USDT
- Вывод каждую неделю
- Комиссия до 5 лет за каждого referral
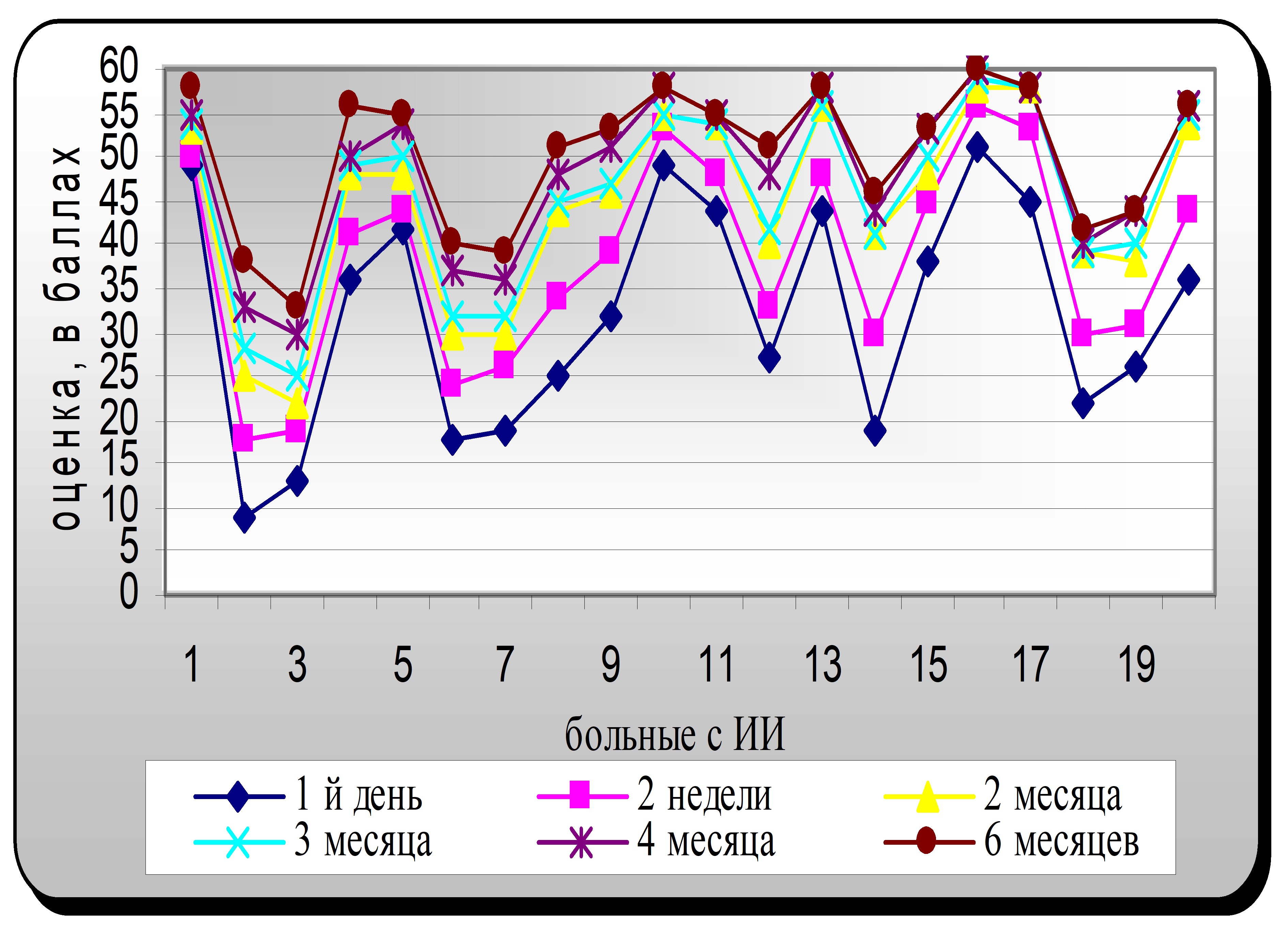
Рисунок 5.Оценка тяжести инсульта по Скандинавской шкале в течении 6 месяцев, при стандартном лечении ИИ.
Таблица № 3. Оценка тяжести инсульта по Скандинавской шкале в течении 6 месяцев, при стандартной лечении ИИ
Кол-во больных | 1- й день | Через | |||
2 недели | 2 месяца | 4 месяца | 6 месяцев | ||
1 | 49 | 50 | 53 | 55 | 58 |
2 | 9 | 18 | 25 | 33 | 38 |
3 | 13 | 19 | 22 | 30 | 33 |
4 | 36 | 41 | 48 | 50 | 56 |
5 | 42 | 44 | 48 | 54 | 55 |
6 | 18 | 24 | 30 | 37 | 40 |
7 | 19 | 26 | 30 | 36 | 39 |
8 | 25 | 34 | 44 | 48 | 51 |
9 | 32 | 39 | 46 | 51 | 53 |
10 | 49 | 53 | 55 | 58 | 58 |
11 | 44 | 48 | 54 | 55 | 55 |
12 | 27 | 33 | 40 | 48 | 51 |
13 | 44 | 48 | 56 | 58 | 58 |
14 | 19 | 30 | 41 | 44 | 46 |
15 | 38 | 45 | 48 | 53 | 53 |
16 | 51 | 56 | 58 | 60 | 60 |
17 | 45 | 53 | 58 | 58 | 58 |
18 | 22 | 30 | 39 | 38 | 42 |
19 | 26 | 31 | 38 | 44 | 44 |
20 | 36 | 44 | 54 | 56 | 56 |
На втором месяце у больных ИИ, до лечения ПД антидепрессивным препаратом (АДП), у 4 (20 %) больных отмечался МДЭ и у 8 (40%) больных БДЭ. После назначения АДП Портала в течении 4-х месяцев у 6 (30%) больных БДЭ трансформировался в МДЭ, а у 2 (10 %) сохранялся БДЭ, но с уменьшением оценочного балла в процентах на 37,1 %.
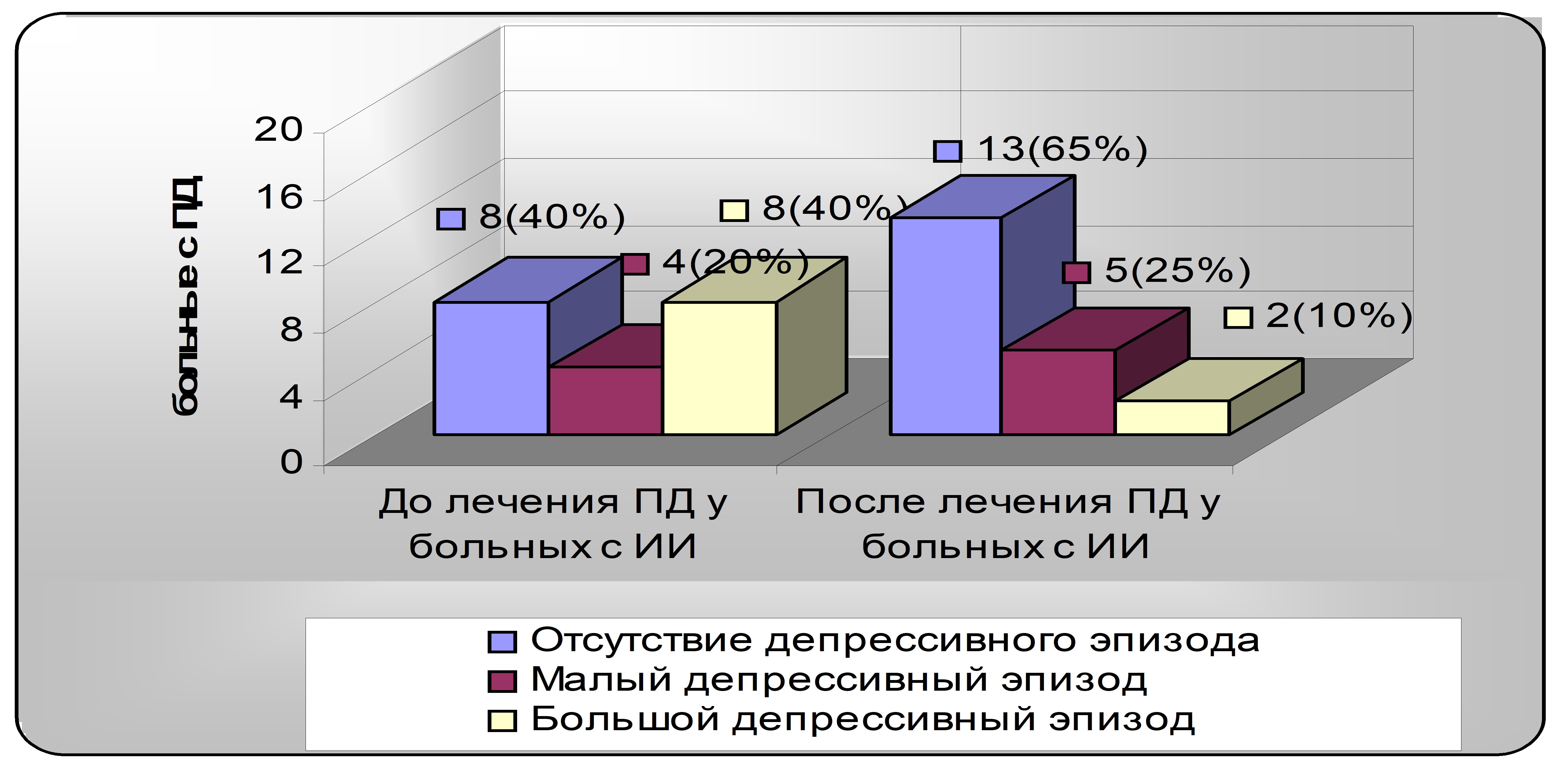
Рисунок 6.Семиотика и динамика депрессивных расстройств по шкале Гамильтона до и после лечения АДП Порталом в течение 6 месяцев.
Выводы
Постинсультная депрессия встречается достаточно часто и имеет хроническое течение. В ранний реабилитационный период инсульта депрессия ассоциирована с его тяжестью, функциональным дефицитом и соматическими заболеваниями. Комплекс реабилитационных мероприятий должен включать эффективные антидепрессанты, так как адекватное лечение постинсультной депрессии достоверно улучшает качество жизни пациентов и положительно влияет на реабилитацию больных.
Список используемой литературы
1.Paolucci S., Antonucci G., et al. Post-stroke depression, antidepressant treatment and rehabilitation results. A case-control study. // Cerebrovascular diseases, 2001; 12: 264-271.
2.Unutzer J., et al. // Int. psychologeriatr., 2000; 12(1): 15-33.
3.Mayberg H. S. Frontal lobe dysfunction in secondary depression. // J. Neuropsychiatry. Clin. Neurosciences, 1994; 6 (4): 428-442.
4.Robinson R. G., Starkstein S. E. Current research in affective disorders following stroke. // J. Neuropsych. Clin. Neuroscinces, 1990; 2 (1): 1-14.
5.Lipsey J. R., et al. Nortriptylin treatment of post-stroke depression: double-blind study. // Lancet, 1984; 1: 297-300.
6.Andersen G., et al. Effective treatment of post-stroke depression with the selective serotonin reuptake inhibitor citalopram. // Stroke, 1994; 25: 1099-1104.
7., , Сорокина после инсульта: опыт применения ципрамила. // Журнал неврологии и психиатрии им. Корсакова C. C., №5, 2002. – C. 36-39.
8.Демиденко при цереброваскулярной патологии. – Л., Медицина, 1989.
9. и др. Депрессия в неврологической практике. – М., Медицина, 1998.
10.Вознесенская в неврологической практике. // В кн.: Лечение нервных болезней, 2000, 1: С. 8-12.
11. и др. Депрессии у соматических больных. – М., 1997.
12. и др. Реабилитация в неврологии: Учеб. пособие. – М., 2000.
13.Лурия нейропсихологии. – М., Изд-во МГУ, 1973.
14. Bogousslavsky J. William Feinberg lecture 2002: emotions, mood, and behaviour after stroke // Stroke.– 2003.– V. 34.– № 4.– P. 1046–1050.
15. Folstein M. F., Maiberger R., McHugh P. Mood disorders as a specific complication of stroke // J. Neurol. Neurisurg. Psychiartr.– 1977.– V. 40.–
P. 1118–1020.
16. Herrmann N., Black S. E., Lawrence J. et al. The Sunnybrook Stroke Study: A prospective study of depressive symptoms and functional outcome // Stroke.– 1998.– V. 29.– P. 618–624.
17. Rammasubu R. Relationship between depression and cerebrovascular disease: conceptual issues // J. affect. Disorders.– 2000.– V. 57.– P. 1–11.
18.Astrm M., Adolfsson R., Asplund K. Major depression in stroke patients: A 3-year longitudinal study // Stroke.– 1993.– V. 24.– P. 976–982.
19.Beblo T., Wallesch C. W., Herrmann M. The crucial role of frontostriatal circuits for depressive disorders in the postacute stage after stroke // Neuropsychiatr., Neuropsychol. Behav. Neurol.– 1999.– V. 12.– № 4.– P. 236–246.
20.Chemerinski E., Robinson R. G. The neuropsychiatry of stroke // Psychosomatics.– 2000.– V. 41.– P. 5–14.
21.Haroon E., Kumar A. The clinical neuroscience of poststroke depression // Cur. Neuropharmacol.– V. 2.– № 4.– P. 353–362.
22.Mayberg H. S., Robinson R. G., Wong D. F. PET imaging of cortical S2 receptors after stroke: lateralized changes and relationship to depression // Am. J. Psychiatr.– 1988.– V. 145.– P. 937–943.
23.Morris P. L., Shields R. B., Hopwood M. J. et al. Are there two depressive syndromes after stroke // J. Nerv. Ment. Dis.– 1994.– V. 182.– P. 230–234.
24.Narushima K., Kosier J. T., Robinson R. G. A reappraisal of poststroke depression, intra– and inter-hemispheric lesion location using meta-analysis // J. Neuropsychiatr. clin. Neurosci.– 2003.– V. 15.– P. 422–430.
25.Dam H., Pedersen H. E., Ahlgren P. Depression among patients with stroke // Acta. Psychiatr. scand.– 1989.– V. 80.– P. 118–124.
26.Williams L. S., Chose S. S., Swindle R. W. Depression and other mental health diagnoses increase mortality risk after ischemic stroke // Am. J. Psychiatr.– 2004.– V. 161.–№ 6.– P. 1090–1095.

|
Из за большого объема этот материал размещен на нескольких страницах:
1 2 3 4 5 |
